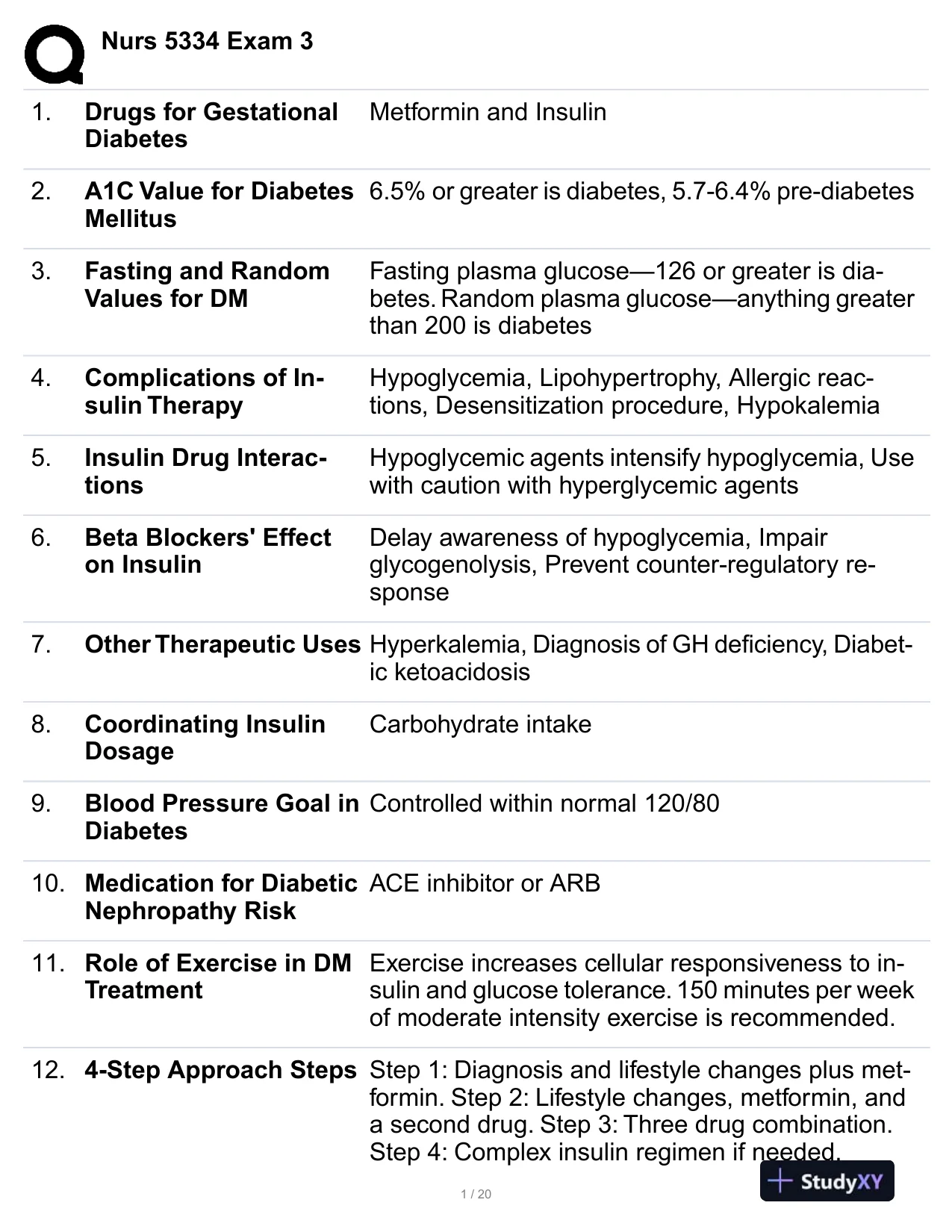
 Nurs 5334 Exam 31.Drugs for GestationalDiabetesMetformin and Insulin2.A1C Value for DiabetesMellitus6.5% or greater is diabetes, 5.7-6.4% pre-diabetes3.Fasting and RandomValues for DMFasting plasma glucose—126 or greater is dia-betes. Random plasma glucose—anything greaterthan 200 is diabetes4.Complications of In-sulin TherapyHypoglycemia, Lipohypertrophy, Allergic reac-tions, Desensitization procedure, Hypokalemia5.Insulin Drug Interac-tionsHypoglycemic agents intensify hypoglycemia, Usewith caution with hyperglycemic agents6.Beta Blockers' Effecton InsulinDelay awareness of hypoglycemia, Impairglycogenolysis, Prevent counter-regulatory re-sponse7.Other Therapeutic UsesHyperkalemia, Diagnosis of GH deficiency, Diabet-ic ketoacidosis8.Coordinating InsulinDosageCarbohydrate intake9.Blood Pressure Goal inDiabetesControlled within normal 120/8010.Medication for DiabeticNephropathy RiskACE inhibitor or ARB11.Role of Exercise in DMTreatmentExercise increases cellular responsiveness to in-sulin and glucose tolerance. 150 minutes per weekof moderate intensity exercise is recommended.12.4-Step Approach StepsStep 1: Diagnosis and lifestyle changes plus met-formin. Step 2: Lifestyle changes, metformin, anda second drug. Step 3: Three drug combination.Step 4: Complex insulin regimen if needed.1 / 20
Nurs 5334 Exam 31.Drugs for GestationalDiabetesMetformin and Insulin2.A1C Value for DiabetesMellitus6.5% or greater is diabetes, 5.7-6.4% pre-diabetes3.Fasting and RandomValues for DMFasting plasma glucose—126 or greater is dia-betes. Random plasma glucose—anything greaterthan 200 is diabetes4.Complications of In-sulin TherapyHypoglycemia, Lipohypertrophy, Allergic reac-tions, Desensitization procedure, Hypokalemia5.Insulin Drug Interac-tionsHypoglycemic agents intensify hypoglycemia, Usewith caution with hyperglycemic agents6.Beta Blockers' Effecton InsulinDelay awareness of hypoglycemia, Impairglycogenolysis, Prevent counter-regulatory re-sponse7.Other Therapeutic UsesHyperkalemia, Diagnosis of GH deficiency, Diabet-ic ketoacidosis8.Coordinating InsulinDosageCarbohydrate intake9.Blood Pressure Goal inDiabetesControlled within normal 120/8010.Medication for DiabeticNephropathy RiskACE inhibitor or ARB11.Role of Exercise in DMTreatmentExercise increases cellular responsiveness to in-sulin and glucose tolerance. 150 minutes per weekof moderate intensity exercise is recommended.12.4-Step Approach StepsStep 1: Diagnosis and lifestyle changes plus met-formin. Step 2: Lifestyle changes, metformin, anda second drug. Step 3: Three drug combination.Step 4: Complex insulin regimen if needed.1 / 20Preview Mode
This document has 20 pages. Sign in to access the full document!