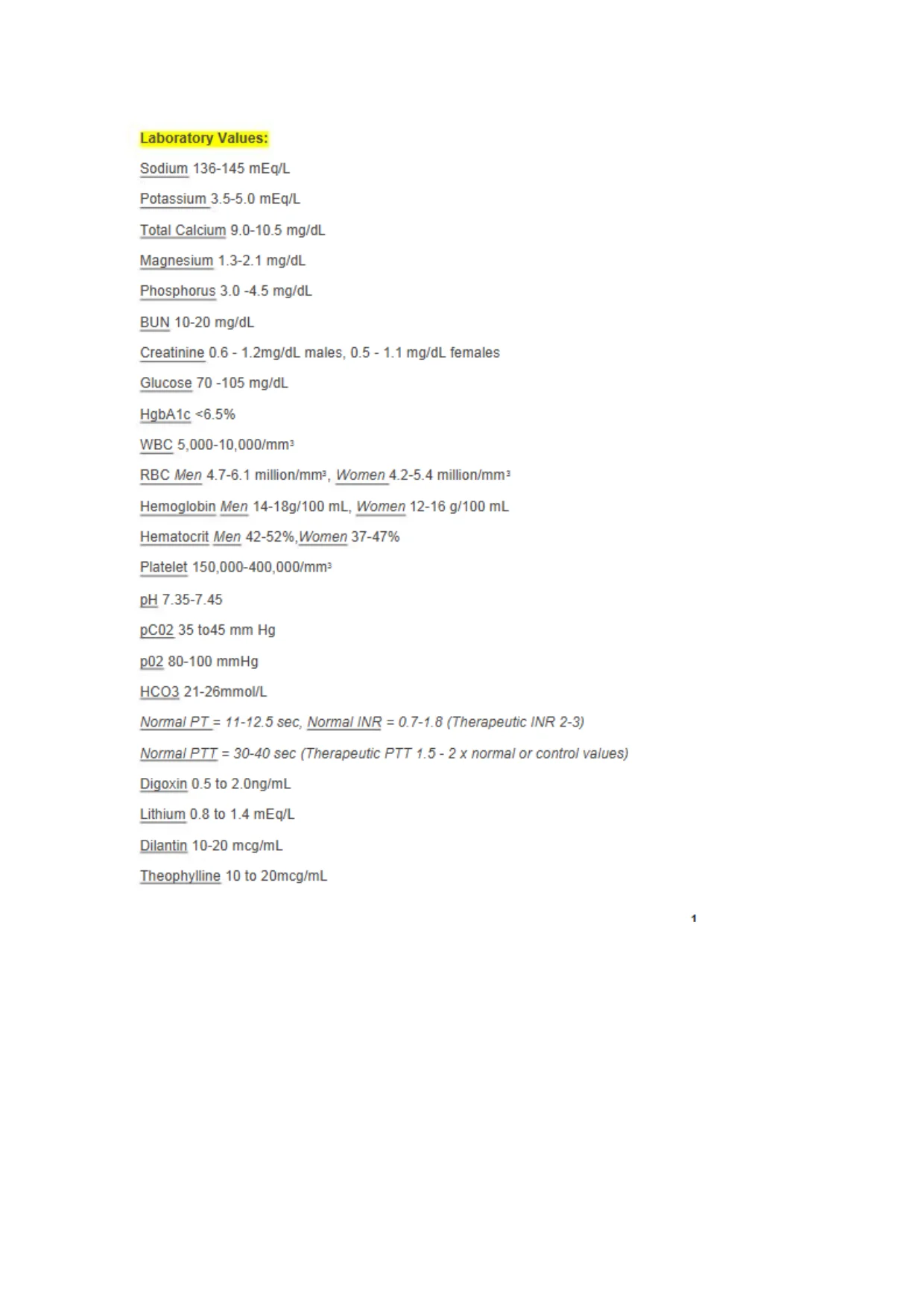
 Laboratory Values:Sodium 136-145 mEq/LPotassium 3.5-5.0 mEq/LTotal Calcium 9.0-10.5 mg/dLMagnesium 1.3-2.1 mg/dLPhosphorus 3.0 -4.5 mg/dLBUN10-20 mg/dLCreatinine 0.6 - 1.2mg/dL males, 0.5 - 1.1 mg/dL femalesGlucose 70-105 mg/dLHgbAlc <6.5%WBC 5,000-10,000/mm--RBCMen4.7-6.1 million/mm-:Women4.2-5.4million/mm2Hemoglobin Men 14-18g/100 mL, Women 12-16 g/100 mLHematocritMen 42-52%,Women37-47%Platelet 150,000-400,000/mnrPpH7.35-7.45pC02 35 to45mm Hgp02 80-100 mmHgHCO3 21-26mmol/LNormal PT = 11-12.5sec,Normal INR = 0.7-1.d (Therapeutic INR 2-3)Normal PTT = 30-40 sec (Therapeutic PTT 1.5- 2 x normal or control values)Digoxin 0.5 to 2.0ng/mLLithium 0.8 to 1.4 mEq/LDilantin 10-20 mcg/mLTheophylline 10 to 20mcg/mL1
Laboratory Values:Sodium 136-145 mEq/LPotassium 3.5-5.0 mEq/LTotal Calcium 9.0-10.5 mg/dLMagnesium 1.3-2.1 mg/dLPhosphorus 3.0 -4.5 mg/dLBUN10-20 mg/dLCreatinine 0.6 - 1.2mg/dL males, 0.5 - 1.1 mg/dL femalesGlucose 70-105 mg/dLHgbAlc <6.5%WBC 5,000-10,000/mm--RBCMen4.7-6.1 million/mm-:Women4.2-5.4million/mm2Hemoglobin Men 14-18g/100 mL, Women 12-16 g/100 mLHematocritMen 42-52%,Women37-47%Platelet 150,000-400,000/mnrPpH7.35-7.45pC02 35 to45mm Hgp02 80-100 mmHgHCO3 21-26mmol/LNormal PT = 11-12.5sec,Normal INR = 0.7-1.d (Therapeutic INR 2-3)Normal PTT = 30-40 sec (Therapeutic PTT 1.5- 2 x normal or control values)Digoxin 0.5 to 2.0ng/mLLithium 0.8 to 1.4 mEq/LDilantin 10-20 mcg/mLTheophylline 10 to 20mcg/mL1Preview Mode
This document has 48 pages. Sign in to access the full document!